


A Historical Autopsy of George Washington's Death
When blood-letting was common and commonsensical

One of the most important concepts one learns during training as a professional historian is the “Whig interpretation of history,” which refers generally to “oversimplified narratives that achieve drama and apparent moral clarity by interpreting past events in light of [the] present...” Historians term such narratives as teleological: that is, narratives which judge the past with reference to values and beliefs of the present.
Applied to the history of medicine, the Whig interpretation often manifests in the form of narratives where the methods of treatment used by humans in the past are described as “primitive” and “barbaric” procedures which were later— and this is where the teleology comes in — dramatically and triumphantly conquered by modern medical ideas and procedures in the mid-1800s and after. While that is a fun story to tell if one wants a convenient, simplified narrative, it leaves out much of the richness of the human aspects of this history. It ignores the historical fact that those “primitive” procedures were part of mainstream medical ideas for hundreds of years across cultures and societies. In its fixation on the present world, it completely misses the point that for people in the past, most of those treatments made sense and “worked.”
Some years ago, I was a teaching assistant for an excellent course taught by Professor David Jones at Harvard, titled “(How) Does Medicine Work?” Among the many illuminating ideas we discussed was that to historians, it is more interesting to understand why in the past certain therapeutic procedures and drugs were championed and thought to “work,” than to understand why those procedures/drugs “do not work” according to contemporary concepts. (Unfortunately, this wonderful curiosity and inquisitiveness about the past is often wrongly considered by many as some kind of approval or romanticization of what was done in the past, but that’s a topic for another essay.)
In their quest to better understand healthcare in the past, historians have produced copious literature on the procedure that perhaps best defines medical treatment in the premodern era— bloodletting. During medical training a student might read at most a sentence or two about it: after all, bloodletting is something that has long been abandoned as a discredited medical idea. But during training in the history of medicine and science, one reads many articles and monographs about it: after all, bloodletting is something that was a common and trusted medical procedure for more than two thousand years in several human societies. Fortunately, I have been both a medical student and a history student, and that has helped me learn from both of these wonderful worlds.
George Washington’s death:
A quick Google search for George Washington’s death tells us that “gruesome” things happened during his final hours. But in Professor Jones’s course, we took a less dramatic approach and looked at Washington’s death in its proper historical context: firmly as part of the social, cultural, and medical milieu of the late 1700s (he died in 1799).
Some basic facts first. As David Morens describes in a 1999 article:
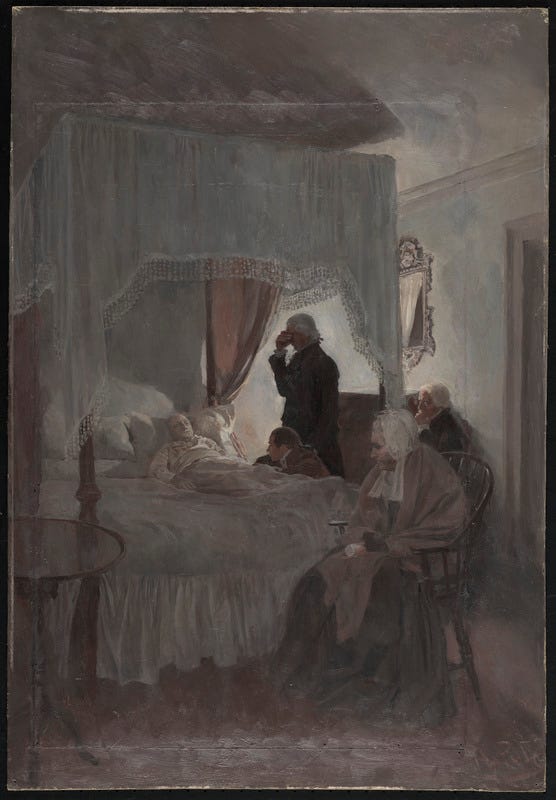
“On Friday, December 13, Washington had “taken a cold,” with mild hoarseness. At 2 the next morning, he awoke and had difficulty breathing. By 6 a.m., he was febrile, with throat pain and respiratory distress. Unable to swallow, he spoke with difficulty. His aide, Colonel Tobias Lear, sent for Craik and bloodletter George Rawlins. At about 7:30 a.m., Rawlins removed 12 to 14 oz (355 to 414 ml) of blood, with Washington requesting additional bloodletting.”
While many popular accounts give the impression that Washington’s “overenthusiastic” physicians almost “bled” him to death, or made the “wrong” decisions, we can see from the above excerpt that he had faith in the procedure and even voluntarily requested it to be done.
“[Later in the day] After the fourth bloodletting, Washington’s condition improved, and he was able to swallow. He examined his will… Around 5 p.m., Washington again sat up in a chair but soon returned to bed and was helped into an upright position. He continued to struggle for air, and his condition began to deteriorate. At 8 p.m., the physicians applied blisters of cantharides to his feet, arms, and legs and then applied wheat-bran cataplasms (poultices) to his throat. His condition deteriorated further. At around 10 p.m., Washington whispered burial instructions to Lear.”
All in all, the bed-ridden George Washington, first President of the United States, had about 2.5 quarts (around 2.4 liters) of blood drawn out of his body in the span of 12 hours. That’s nearly half of an average adult human’s entire blood volume. Despite these “heroic” efforts, though, Washington died in the night around 10.30 pm.
Today, this all seems pretty bizarre. The primary complaint Washington had was throat discomfort and fever (scholars believe now that he had developed what we call “acute epiglottitis”), but the main treatment he received, even demanded, was… bloodletting. Three physicians in total were around him that day — all of them elite doctors of the time— supervising everything. What were they thinking?!

The rationale behind bloodletting:
Among the most cited articles in the history of medicine literature is a 1977 one by historian Charles Rosenberg, “The Therapeutic Revolution: Medicine, Meaning, and Social Change in Nineteenth-Century America.” In it he wrote:
Therapeutics is after all a good deal more than a series of pharmacological or surgical experiments. It involves emotions and personal relationships and incorporates all of those cultural factors which determine belief, identity, and status. The meaning of traditional therapeutics must be sought within a particular cultural context… Individuals become sick, demand care and reassurance, are treated by designated healers.
Basically, bloodletting made sense to Washington (the patient) and to his physicians because it fit in well with the prevailing notions of how the human body works. The body was thought of not as a collective of many kinds of discrete tissues and organs as we do today, but as a single whole in which there was “a system of intake and outgo — a system which had necessarily to remain in balance if the individual were to remain healthy… Equilibrium was synonymous with health, disequilibrium with illness.” These concepts of equilibrium can be traced (in the American and European context) to classical Greek and Roman medical ideas of the four humors representing four natural elements that had to be maintained in a perfect balance within the body.
The American physician in 1800 had no diagnostic tools beyond his senses and it is hardly surprising that he would find congenial a framework of explanation which emphasized the importance of intake and outgo, of the significance of perspiration, of pulse, of urination and menstruation, of defecation… These were phenomena which [the] physician, the patient, and patient’s family could see, evaluate, scrutinize for clues to the sick individual’s fate… Drugs [and medical procedures] had to be seen as adjusting the body’s internal equilibrium, and the drug’s action had, if possible, to alter these visible products of the body’s otherwise inscrutable internal processes.
This prevalent understanding of ill health as disequilibrium meant that the best way to heal was to make some adjustments to the humors in the body and bring it back an equilibrium state.
So how does one do that? Well, by getting rid of excess humors or halting the loss of scarce humors. Hence physicians advised therapeutic modalities like emetics (which caused vomiting) and bloodletting. And how to make sure that an adjustment toward equilibrium is indeed taking place internally? Well, by using the then-current technology: one’s own human senses. As Rosenberg writes, the treatment needed to produce “visible and predictable physiological effects; purges purged, emetics vomited, opium soothed pain and moderated diarrhea. For example, bloodletting seemed obviously to alter the body’s internal balance, as seen both by the change in the pulse and other outward signs, and the sheer visibilty of the blood drawn out. At the same time, “the product elicited — urine, feces, blood, perspiration — could be conveniently examined so as to shed [additional] light on the body’s internal state.”
People who lived in 1700s America (and other parts of the world too), did not find it hard to believe that bloodletting was a legitimate therapeutic procedure which, as any therapeutic procedure in gneeral, sometime sworked and sometimes did not work. The many reasons why people believed bleeding (bloodletting, plus, eg, the application of leeches and other methods of drawing blood) to be a completely rational therapy can be summarized as follows:
It rarely killed (patients who did die despite the procedure seldom died right after bloodletting).
In the absence of any way to look into the intact human body, blood was considered a very powerful marker of the body’s internal workings and state of affairs.
For both physicians and patients, bloodletting provided a sense of “something being done” to take control of the situation and effect improvements in it. Moreover, this “something” had a long and rich medical tradition behind it.
Since many ailments are self-limiting, the recovery of the sick person after a certain period of time provided an ex post facto validation of the therapy. Non-recovery was most often interpreted as the disequilibrium being just too strong, or the bleeding done inadequately or improperly.

So did it “really” work?
A few years ago, with only medical training informing my worldview, I would quite assertively have answered this with an instantaneous No. I did not have the “historical empathy” for George Washington and his doctors (and for past therapeutics in general) that I have today.
To revisit what Rosenberg said in the first extract above, therapeutics involved “a good deal more than a series of pharmacological or surgical experiments, [including] emotions and personal relationships.” Unlike most of us in the present, folks in the past were not looking for precise diagnoses and certified treatment protocols from their physicians. They were mainly looking for prognosis and reassurance. In that context, the very act of a doctor doing something seemingly powerful and mainstream made the patient feel to be in “good hands” and on the way to potential recovery. In the patient-physician encounter, as long as the doctor confidently predicted a trajectory either of full or partial recovery (or even non-recovery), and appeared to do everything in their power to make the patient feel better, things made sense and were thought generally to “work” (clearly, this general rule applies even today).
In the case of Washington in 1799, mainstream medical opinion and even public opinion debated whether the doctors had bled him “too much,” but the very act of bloodletting was not under any serious attack (that happened much later). Washington of course died, and so for the patient George Washington in 1790s America, bloodletting did “not work.” But it did not work only to the extent that we would, for example, say that an appendectomy did not work for a patient with an acutely inflamed appendix who ultimately died despite the surgery. That is, just because this patient died, people today would not lose confidence in the value of surgery and appendectomy; instead, we would just say that it didn’t work in the medical context of that particular patient.
To sum it all up, we often do a disservice to people in the past when we mock their ideas as “primitive” or “irrational” In the case of bloodletting, for example, historians have shown that people had perfectly rational reasons — according to the beliefs and ideas of those times — for trusting it. When we ridicule people in the past for their ideas and beliefs without fully exploring their particular contexts, it is our capacity of comprehension, not theirs, that ultimately is in the dock. (We should tread with care, of course, when applying such a view of the past to something with multiple layers of complexity such as, say, the Witch Trials involving midwives, where the reasons were less “rational” and medical, and more about controlling and exerting power over women; or to something such as colonialism, which was less about “civilizing” so-called barbaric people, and more about enriching and empowering the ostensible civilizers.)